Brain Cancer & Behaviour
Trigger Warning This case study includes content related to depression and suicide. If you need help, call Lifeline on 13 11 14 or talk with a counsellor online.
The Case
The paper on which this case study is based can be found here.
Patient Details
AGE: 28
SEX: male
PRESENTED WITH: headache and personality changes but became increasingly pensive and indifferent.
Investigation
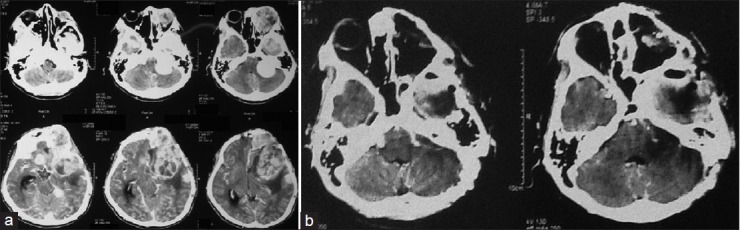
CT scan was performed, which discovered a tumour in the left side of his brain. This tumour was removed and he was diagnosed with meningioma.
A year later, the patient returns and presents with a headache and a lump on his scar from the operation. A CT scan showed that there was a mass on in the same place as the first tumour.
His behaviour also changed, in that he was now talking to himself and was quite angry. He was also withdrawn and wanted to be alone.
He underwent a similar operation as before and the tumour was removed. It was found to be the same type of cancer – meningioma. He was then scheduled to have that area of his brain removed 3 weeks later, in hope that all cancerous cells could be removed.
After the surgery, his behavioural changes reduced but didn’t disappear. Ten days before his operation, the patient became very aggressive, erratic and had suicidal tendencies. He was then referred to the psychiatric department. There, he was diagnosed with mild depression and was given psychotherapy.
Several days after his surgery, the patient was discharged with improvement in his physical and psychological condition. He no longer had suicidal tendencies.
—
© 2014 Arifin MZ, from Surg Neurol Int. 2014; 5: 174.
What are brain cancers?
Cancers in the brain can be primary or secondary. Primary cancers start in the brain and usually do not spread to other parts of the body, whereas, secondary cancer are tumours that start from another part of the body and travel to the brain.
There are more than 40 types of brain cancers, with two main groups: benign and malignant.
- Benign tumours are slow growing and are unlikely to spread. They include meningiomas and neuromas.
- Malignant tumours grow faster than benign tumours and can spread to other parts of the body. They include astrocytomas, oligodendrogliomas and glioblastomas.
Here is a useful overview of brain cancer.
Who gets brain cancer?
According to the Australian Cancer Research Foundation, brain cancer is more commonly diagnosed in men (1 in 100) before the age of 85 than women (1 in 151). In 2009, 1,596 new cases of brain cancer were diagnosed in Australia. The five-year survival rate for Australians diagnosed with brain cancer is 21.9%. In 2010, there were 1,247 deaths from brain cancer.
These statistics were sourced from here.
What is a meningioma?
Meningiomas are tumours that arise from the meninges – membranes or tissue that surround the brain and the spinal cord. Meninges are very important in protecting the central nervous system. These types of cancers are most common in older women.
Why does the patient have behavioural or personality changes?
As a brain cancer grows, it puts pressure on the surrounding tissue, thereby affecting brain function. Symptoms of brain cancers depend on the location of the cancer and the size of the tumour, as each area of the brain has different functions. In saying this, many areas interact with each other and the brain is thought to have an integrated function, this means that damage to one area of the brain can result in symptoms that are indirectly related to its function. For example...
- The frontal lobe of the brain is important for cognitive processing. It controls personality, behaviour, emotions, movement, motivation, problem solving and memory.
- The parietal lobe has many functions, including visual interpretation, spatial awareness and the sense of touch.
In this case, the patient’s tumour was putting pressure on his frontal lobe, affecting the cells that contribute to personality and mood. Swelling in the brain may also contribute to his headaches and irritability.
Why does the patient feel suicidal?
Almost 40% of brain tumor patients experience meaningful depression... — Arifin et al
Depression may be due to many things.
The tumour itself may be impinging on areas that are involved in suicidal tendencies.
Simply being diagnosed with cancer. The period after diagnosis is one of the times of greatest risk for suicide as patients may feel hopelessness, alone or fear of pain and abandonment. Paired with stress of treatment and financial difficulties, these feelings can lead to suicidal thought.
The harsh side effects of cancer treatment, such as chemotherapy and radiotherapy could cause further damage and affect brain function. Changes in hormonal levels can also affect the brain, resulting in mood disturbances. In addition, lifestyle changes that are associated with worsening of symptoms or with therapy further feed into depression.