Common Cancers
Breast Cancer
Structure & Function of Breasts
The female breast is mostly made up of a collection of fat cells called adipose tissue. This tissue extends from the collarbone down to the underarm and across the middle of the ribcage.
A healthy human female breast is made up of 12-20 sections called lobes. Each of these lobes is made up of many smaller lobules, the gland that produces milk in nursing women. Both the lobes and lobules are connected by milk ducts, which act as stems or tubes to carry the milk to the nipple.
Within the adipose tissue is a network of ligaments, fibrous connective tissue, nerves, lymph vessels, lymph nodes and blood vessels.
The US National Breast Cancer Foundation has an excellent video on this topic.
The lymphatic system, which is part of the immune system, is a network of lymph vessels and lymph nodes running throughout the entire body. Similar to how the blood circulatory system distributes elements throughout the body, the lymph system transports disease-fighting cells and fluids. Clusters of bean-shaped lymph nodes are fixed in areas throughout the lymph system and act as filters by carrying abnormal cells away from healthy tissue.
What is breast cancer?
Breast cancer is a malignant tumour that originates in the cells of the breast.
Breast cancer can start in the ducts or lobules of the breast. If the cancer cells stay in the ducts and lobules of the breast, the breast cancer is said to be non-invasive. If the cancer cells spread to surrounding tissue, the breast cancer is said to be invasive.
Most breast cancers are ductal carcinomas. Ductal carcinomas originate in the ducts that carry milk to the nipple and are malignant. Less common are lobular carcinomas. Lobular carcinomas form within the cells that line the lobules which produce milk.
Breast cancer is the most commonly diagnosed cancer among women in Australia. Breast cancer occurs predominantly in females, although men can also develop the disease. 1 in 8 women will develop breast cancer in their lifetime. It is more common in women aged over 60, although around ¼ of women with breast cancer are younger than 50, and it can occur at any age.
Types of breast cancer
Ductal carcinoma in situ (DCIS) DCIS occurs when abnormal changes take place in the cells which form the milk ducts of the breast. DCIS is a non-invasive breast cancer, meaning the abnormal or cancerous cells are contained inside the milk ducts and have not spread to the surrounding tissue. It is not a fatal type of cancer unless it turns invasive. Women at any age can develop DCIS, however, most women are between 50 and 59 years. DCIS can also develop in men; however, this is very rare.
Invasive ductal carcinoma Invasive ductal carcinoma is the most common type of breast cancer in Australia. It starts in the cells that line the ducts of the breasts (known as DCIS) and has begun to spread into the surrounding breast tissue.
Lobular carcinoma in situ (LCIS) Lobular carcinoma in situ (LCIS) is the name for abnormal cells that are contained in the lobules of the breast (where milk is produced). In LCIS, the abnormal cells do not spread to other parts of the breast or body so it is not considered pre-malignant. Occasionally, because of this fact, LCIS is referred to as a ‘neoplasia’ (a collection of abnormal cells), rather than a typical carcinoma. LCIS does not show up on mammogram results and usually does not cause symptoms. Most cases of LCIS are found when a woman has a biopsy for another reason. Most women are not aware of any symptoms at the time of diagnosis. LCIS is more common in women who have not yet gone through menopause. Men can develop LCIS but this is very rare.
Invasive lobular carcinoma Invasive lobular carcinoma occurs when cancer has started in the cells that line the lobules of the breast (LCIS) and has now spread into the surrounding breast tissue. Invasive lobular carcinomas can develop in women of any age; however, it is most common in women between the ages of 45 and 55. If you are diagnosed with invasive lobular breast cancer in one breast, there is a slightly higher risk of getting it in the other breast in the future. There are different subtypes of invasive lobular carcinoma. In its most typical or “classic” form, ILC is made up of small cancer cells that invade the fatty tissue and ligaments that surround the milk ducts and lobules inside the breast, as well as the surrounding blood and lymph vessels.
Which of the following statements about breast cancer is correct?
Lung Cancer
Structure & function of lungs
For an alternative overview of the topic, see this page from Cancer Council Victoria.
Our lungs are the main organs we use for breathing and they make up part of what is called the respiratory system.
The airways to each lung consist of large airways (bronchi) and small airways (bronchioles). Air that we breathe in first goes into the nose or mouth, down the trachea and then into the bronchi and bronchioles. Alveoli are tiny air sacs at the ends of bronchioles, which pass oxygen into the blood and collect the waste gas, carbon dioxide, from the blood. When we breathe out, carbon dioxide is released back into the atmosphere.
Our lungs look like two large, cone-shaped sponges: the lungs are composed of sections called lobes (left lung has two lobes, right lung has three lobes). The lungs rest on the diaphragm, which is a wide, thin muscle that helps with breathing.
A number of structures lie in the space between the lungs including:
The heart and large blood vessels
The windpipe (trachea), the tube that carries air into lungs
The oesophagus (the tube that carries food from the mouth to the stomach)
Lymph nodes that collect lymph fluid and foreign matter from the lungs
The lungs are covered by two layers of a thin sheet of tissue called the pleura, which is about as thick as plastic cling wrap. Its inner layer (the visceral layer) is attached to the lungs and its outer layer (the parietal layer) lines the chest wall and diaphragm.
What is lung cancer?
Lung cancer is a malignant tumour in the tissue of one or both of the lungs. A primary cancer starts in the lungs, while a secondary or metastatic cancer starts somewhere else in the body and spreads to the lungs.
Types of lung cancer
There are several types of lung cancer, which are classified according to the type of cells affected. Each type of non-small cell lung cancer has different kinds of cancer cells. The cancer cells of each type grow and spread in different ways. The types of non-small cell lung cancer are named for the kinds of cells found in the cancer and how the cells look under a microscope.
A similar overview has been compiled by the Australian Cancer Research Foundation. See here.
Small cell carcinoma This type of cancer accounts for about 12 per cent of all lung cancer cases. It usually arises from epithelial cells that line the surface of the middle of the lung. This type of cancer is associated with a history of smoking. Sometimes the cancer will stay confined to the place in the chest in which it originated; this cancer type is described as ‘limited’. Once the cancer has spread it is described as ‘extensive’.
More detailed information can be found at this page from the US National Cancer Institute.
Non-small cell carcinoma This cancer type accounts for over 60 per cent of lung cancer and is the most common form. It consists of a different group of cancers that tend to grow and spread more slowly than small cell carcinomas. There are three main types of non-small cell carcinomas. They are:
Squamous cell lung cancer The most common type of non-small cell carcinomas. Squamous cell lung cancer develops from the cells that line the airways and it is often found near the centre of the lung in one of the main airways.
Adenocarcinoma Develops from the cells that line the airways that produce mucus (phlegm). It is often found in the outer areas of the lungs (in alveoli).
Large cell carcinoma Called large cell carcinoma because the cells look large and rounded under a microscope. This type of lung cancer does tend to grow rapidly.
While not strictly a lung cancer, mesothelioma is a rare chest and abdominal lining cancer mainly affecting people exposed to asbestos particles.
COPD
COPD: Chronic obstructive pulmonary disease
An obstructive lung disease is characterized by difficulty with/increased effort during exhalation. Examples of obstructive lung disease include:
- Asthma
- Emphysema
- Chronic bronchitis
- COPD
While COPD is generally caused by an environmental factor, e.g. cigarette smoke, there are also genetic causes. One such genetic condition called alpha-1 antitrypsin can lead to lung damage and may increase the risk of COPD (may require concurrent exposure to some environmental factor, e.g. cigarette smoke).
You can explore the NIH page on COPD here.
So what is the relationship between COPD and lung cancer?
- Both are caused by cigarette smoking and more research continues to suggest there is a link between these two conditions, apart from their common cause.
- Smokers with COPD are five times more likely to develop lung carcinoma than smokers with normal lung function.
- COPD patients have twice the risk of lung cancer development, even when excluding other factors, e.g. some environmental mutagen.
- There is a high prevalence of lung cancer in COPD patients. This means, in a random sample, e.g. 100 people (50 COPD patients, 50 patients with normal lung function), there will be more lung cancer patients in the COPD group.
A more detailed discussion of the relationship between COPD and lung cancer can be found here.
Metastasis
Like many other cancers, lung cancer is capable of metastasis to other organs. Indeed, many of us have likely heard that lung cancer is extremely aggressive, with 30-40% of patients with non-small-cell lung cancer (NSCLC) exhibiting some form of metastatic disease by the time of diagnosis.
Locations of metastasis are variable among NSCLC patients. Variable metastatic manifestations affect treatment plans, effectiveness of treatment, prognosis, and survival.
Metastatic locations include, but are not limited to:
- Pleural/pericardial fluid
- Pleura
- Lungs
- Extrathoracic lymph nodes
- Bone
- Brain
- Adrenal glands
- Liver
Exactly which metastatic location indicates a poor prognosis is constantly debated. Some studies suggest that brain metastasis is a poor prognostic marker, while other studies suggest that liver metastasis indicates an even worse prognosis. Since metastasis generally characterizes the systemic damage and aggressiveness of a cancer, it is safe to say that doctors must at least take into consideration a patient's metastatic location when developing aggressive treatment plans.
A more detailed discussion on metastatic location and impacts on survivability, including the statistics, can be found here.
Symptoms
This section discusses the general symptoms of lung cancer. It is important to note that there may be differences in symptoms between types of lung cancer (e.g. small cell carcinoma vs. non-small cell carcinoma).
- Dry cough
- Changing chronic cough
- Chest pain
- Breathlessness
- Recurrent pneumonia or bronchitis
- Haemoptysis (coughing up blood or blood-stained mucus)
- Fatigue
- Interestingly, this is the most commonly reported symptom in lung cancer patients. Cancer-related fatigue (CRF) is a problem that affects the quality of life for patients; thus, treatment is important. Treatment of CRF must also address other associated symptoms, e.g. pain, depression, and insomnia, making treatment of CRF a very challenging pursuit. There is not much evidence to support the effectiveness of pharmacological therapies. In fact, other data suggests that alternative remedies and physical exercise are more promising for treatment of CRF.
A more detailed analysis of CRF in lung cancer patients can be found here.
Which of the following statements about lung cancer is correct?
Melanoma
Structure and function of skin
The skin is the largest organ in the body. The skin protects against heat, sunlight, injury and infection. The skin also helps control body temperature and stores water, fat and vitamin D. The skin consists of three layers: the epidermis, the dermis and the subcutis.
The epidermis is the top layer of the skin. It is very thin. It protects the deeper layers of skin and the organs of the body from the environment. The main types of cells in the epidermis include:
Squamous cells are flat cells in the upper part of the epidermis that are constantly shed as new ones form.
Basal cells are in the lower part of the epidermis called the basal cell layer. These cells constantly divide to form new cells to replace the squamous cells that wear off the skin’s surface. As these cells move up in the epidermis, they get flatter, eventually becoming squamous cells.
Melanocytes are the cells that make a brown pigment called melanin, which gives the skin its tan or brown color. Melanin protects the deeper layers of the skin from some of the harmful effects of the sun. For most people, when skin is exposed to the sun, melanocytes make more of the pigment, causing the skin to tan or darken.
The epidermis is separated from the deeper layers of skin by the basement membrane.
The dermis is the middle layer of the skin. It is much thicker than the epidermis. It contains hair follicles, sweat glands, blood vessels, and nerves that are held in place by a protein called collagen, which gives the skin its elasticity and strength.
The subcutis is the deepest layer of the skin. The subcutis and the lowest part of dermis form a network of collagen and fat cells. The subcutis helps the body conserve heat and has a shock-absorbing effect that helps protect the body’s organs from injury.

What is skin cancer?
Melanoma is a cancer that develops in melanocytes. Melanocytes produce melanin to help protect the skin from ultraviolet (UV) radiation. When melanocytes aggregate together in the skin during childhood or adolescence they form a mole. Most moles are quite safe, however sometimes the melanocytes in a mole begin to grow and divide in an uncontrolled way. If they start to grow in an unregulated way, either expanding outwards or down into the lower layers of the skin, they can become a melanoma.
See Cancer Council and US National Cancer Institute for further reading on melanoma.
Melanoma is the most serious form of skin cancer and grows very quickly if left untreated. It can spread to the lower part of your skin (dermis), enter the lymphatic system or bloodstream and then spread to other parts of the body, such as to the lungs, liver, brain or bone.
The most important warning sign for melanoma is a new spot on the skin or a spot that is changing in size, shape, or color. Another important sign is a spot that looks different from all of the other spots on your skin (known as the ugly duckling sign).
The ABCDE rule is another guide to the usual signs of melanoma.
A is for Asymmetry One half of a mole or birthmark does not match the other.
B is for Border The edges are irregular, ragged, notched, or blurred.
C is for Colour The color is not the same all over and may include shades of brown or black, or sometimes with patches of pink, red, white, or blue.
D is for Diameter The spot is larger than 6 millimeters across (about ¼ inch – the size of a pencil eraser), although melanomas can sometimes be smaller than this.
E is for Evolving The mole is changing in size, shape, or color. Melanoma is the fourth most common cancer diagnosed in Australia, which along with New Zealand has the world’s highest incidence rate for melanoma.
![In the lower row from left to right: melanomas showing (A) Asymmetry, (B) a border that is uneven, ragged, or notched, (C) coloring of different shades of brown, black, or tan and (D) diameter that had changed in size. The normal moles in the top row do not have abnormal characteristics (no asymmetry, even border, even color, no change in diameter).<br />—<br />ABCD rule by National Cancer Institute via Skin Cancer Foundation [Public Domain]](assets/Melanomas.jpg)
—
ABCD rule by National Cancer Institute via Skin Cancer Foundation [Public Domain]
Types of melanoma
Melanomas fall into four basic categories:
Superficial spreading melanoma is the most common type, accounting for about 70% of all cases. It is often seen in young people. In this type, melanoma travels along the top layer of the skin for a fairly long time before penetrating more deeply.
Lentigo melanoma is found most often in the elderly, arising on chronically sun-exposed, damaged skin on the face, ears, arms and upper trunk.
Acral lentiginous melanoma usually appears as a black or brown discoloration under the nails or on the soles of the feet or palms of the hands. It spreads superficially before penetrating more deeply. It is the most common melanoma in African-Americans and Asians, and the least common among Caucasians.
Nodular melanoma is usually invasive at the time it is first diagnosed. It is usually black, but occasionally is blue, gray, white, brown, tan, red or skin tone.
Which of the following statements about skin cancer is correct?
Bowel Cancer
Structure & function of the gastrointestinal tract
The gastrointestinal or digestive tract (also known at the GI tract or gut) is the system of organs which remove and process nutrients (vitamins, minerals, carbohydrates, fats, proteins and water) from foods and helps pass waste material out of the body. The gastrointestinal tract is made up of the oesophagus, stomach and the small and large intestines.
For a basic overview of the gastrointestinal tract, click here to watch a YouTube video by CrashCourse.
The oesophagus is the hollow muscular tube that moves food and liquid from the throat to the stomach. The wall of the oesophagus is made up of several layers of tissue, including mucous membrane, muscle and connective tissue.
The stomach is a J-shaped organ in the upper abdomen. The stomach helps in the digestion of food by mixing it with digestive juices and churning it into a thin liquid. After leaving the stomach, partly digested food passes into the small intestine and then into the large intestine.
The small intestine mainly absorbs nutrients from broken down food.
The colon (the first 1.8 metres of the large intestine) mainly absorbs water and the rectum and anal canal (the last 15 centimetres of the large intestine) stores waste material (faeces) until they are passed from the body through the anus. The anal canal ends at the anus, the opening of the large intestine to the outside of the body. The colon and rectum together are known as the large bowel (or large intestine).
What is bowel cancer?
Bowel cancer, also called colorectal cancer, is a cancer of the colon or rectum.
Bowel cancer is a malignant growth that develops most commonly in the lining of the large bowel. Most bowel cancers develop from tiny growths called ‘polyps’. Not all polyps become cancerous. Over time some polyps can become cancerous. Cancer can narrow and block the bowel or cause bleeding. In more advanced cases, the cancer can spread beyond the bowel to other organs.
As most bowel cancers start as polyps, all polyps should be removed to reduce your risk of developing the disease. Almost all polyps can be removed without an operation during the procedure of colonoscopy. Once removed from the bowel, the polyp can no longer develop into cancer. Even if a polyp develops into cancer, in its early stages it can be cured by surgery.
Sometimes bowel cancer runs in families. There are two rare genetic conditions that occur in some families. These cause a small number (5–6%) of bowel cancers.
The Cancer Council and Bowel Cancer Australia have some neat further resources on this topic.
Familial adenomatous polyposis (FAP) This condition causes hundreds of polyps to form in the bowel. If polyps caused by FAP are not removed, they will become cancerous.
Lynch syndrome Previously known as hereditary non-polyposis colorectal cancer (HNPCC), this syndrome is characterised by a fault in the gene that helps DNA repair itself. Having Lynch syndrome increases the risk of developing bowel cancer and other cancers.
![Image of resected colon segment with cancer by <a href="http://www.achsc.org.au/syllabus/3-34/%E2%80%9Dhttps://commons.wikimedia.org/w/index.php?title=User:Bernstein0275&action=edit&redlink=1%E2%80%9D">Bernstein0275</a> [edited] / <a href="https://commons.wikimedia.org/wiki/Category:CC-BY-SA-3.0">CC-BY-SA-3.0</a>](http://www.achsc.org.au/wp-content/uploads/2016/08/800px-Image_of_resected_colon_segment_with_cancer__4_nearby_polyps_plus_schematic_of_field_defects_with_sub-clones.jpg)
Which of the following statements about bowel cancer is correct?
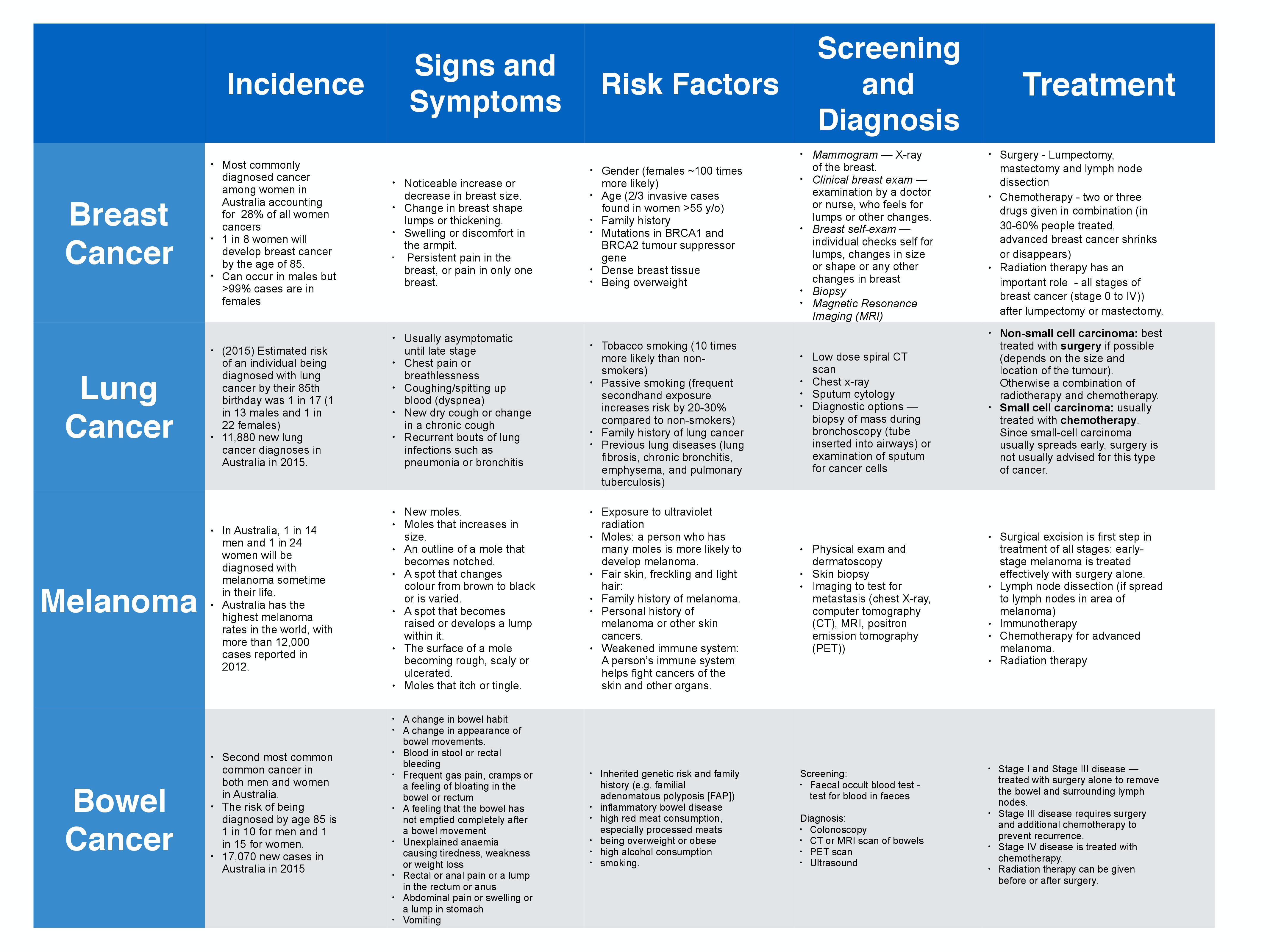
Summary
A pdf of the following table is available for download.
.
Which of the following statements about cancer is INCORRECT?